Nowhere is prompt and effective medical treatment more important than on the battlefield, where injuries are severe and conditions dangerous. Soldiers are vulnerable to many injuries on the battlefield, the most common combat wounds include: Blast wounds caused by landmines, grenades, IEDs (improvised explosive devices), and suicide bombings where the Amputation rates are high. Other are Gunshot and shrapnel wounds and Head injuries and fractured bones. Blast injuries, burns, and other wounds experienced by warfighters often catastrophically damage their bones, skin, and nerves, resulting in months to years of recovery for the most severe injuries and often returning imperfect results. This long and limited healing process means prolonged pain and hardship for the patient, and a drop in readiness for the military.
Blast injuries, burns, and other wounds experienced by warfighters often catastrophically damage their bones, skin, and nerves, resulting in months to years of recovery for the most severe injuries and often returning imperfect results. This long and limited healing process means prolonged pain and hardship for the patient, and a drop in readiness for the military.
Combat wounds are much more complex because of higher contamination, mostly resulting from the environment where the wound occurred. The challenge and complexity of combat wounds are the large wound size and the heavy amount of drainage. Faster wound healing time or surgical closure is indicated because of painful dressing changes and risk of infection. Wound care has evolved immensely throughout the years in the military arena. Today, the military is using the latest technologies, such as digital imaging and telemedicine. This allows them to send combat wound images from the battlefield or to prepare the hospital site for their injured soldier. In previous wars, troops who lost limbs on the battlefield often died from blood loss. But today, better first aid training and faster medevac keep many more troops alive, with a significant number returning to active duty.
The current standard of care when working with a combat wound are:
- Impregnated polyhexamethylene biguanide gauze dressings
- Silver dressings – antimicrobial properties
- Negative pressure wound therapy – less frequent dressing changes, and controls high amounts of exudate
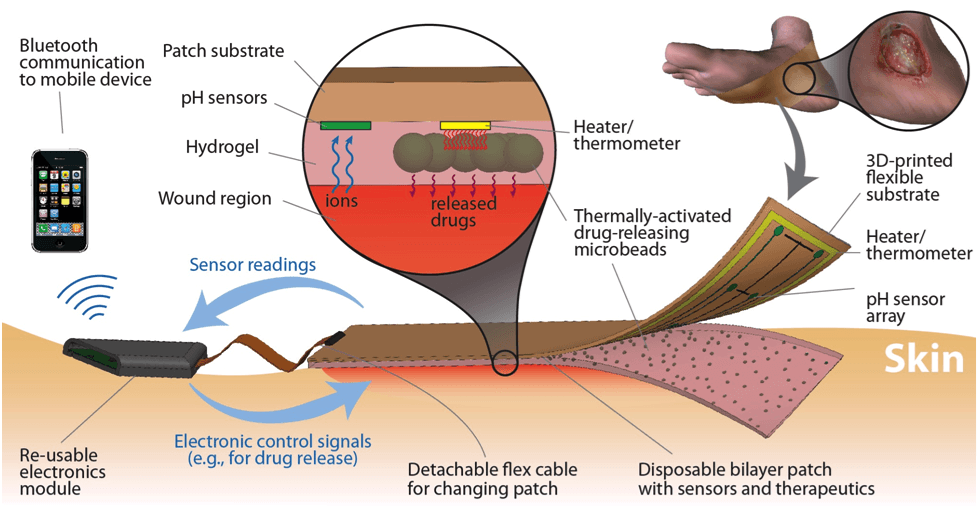
- Moisture sensors – allows dressing decisions without disturbing the dressing
Although recent experimental treatments offer some hope for expedited recovery, many of these new approaches remain static in nature. For instance, some “smart” bandages emit a continuous weak electric field or locally deliver drugs. Alternatively, hydrogel scaffolds laced with a drug can recruit stem cells, while decellularized tissue re-seeded with donor cells from the patient help avoid rejection by the host’s immune system. These newer approaches may indeed encourage growth of otherwise non-regenerative tissue, but because they do not adapt to the changing state of a wound, their impact is limited.
However, these approaches are passive approaches, Under current medical practice, physicians provide the conditions and time for the body to either heal itself when tissues have regenerative capacity or to accept and heal around direct transplants. Most people are familiar with interventions that include casts to stabilize broken bones or transplants of healthy ligaments or organs from donors to replace tissues that do not regenerate. Passive approaches often result in slow healing, incomplete healing with scarring, or, in some unfortunate cases, no healing at all. Blast injuries in particular seem to scramble the healing processes; 23 percent of them will not fully close. Moreover, research shows that in nearly two thirds of military trauma cases — a rate far higher than with civilian trauma injuries — these patients suffer abnormal bone growth in their soft tissue due to a condition known as heterotopic ossification, a painful experience that can greatly limit future mobility.
DARPA launched the Bioelectronics for Tissue Regeneration (BETR) program in 2019 that represent a sharp break from traditional wound treatments, and even from other emerging technologies to facilitate recovery, most of which are passive in nature. The envisioned BETR technology is aimed at speeding warfighter recovery, and thus resilience, by directly intervening in wound healing. DARPA believes that recent advances in biosensors, actuators, and artificial intelligence could be extended and integrated to dramatically improve tissue regeneration. To achieve this, the new Bioelectronics for Tissue Regeneration (BETR) program asks researchers to develop bioelectronics that closely track the progress of the wound and then stimulate healing processes in real time to optimize tissue repair and regeneration. DARPA believes that recent advances in biosensors, actuators, and artificial intelligence could be extended and integrated to dramatically improve tissue regeneration.
To do this, researchers will build an adaptive system that uses actuators to biochemically or biophysically stimulate tissue, sensors to track the body’s complex response to that stimulation, and adaptive learning algorithms to integrate sensor data and dictate intervention to the actuators. After establishing this closed-loop control over physiological processes, BETR researchers will integrate these devices into a single platform that guides the tissue in real-time along an optimal growth pathway.
Paul Sheehan, the BETR program manager, described his vision for the technology as “not just personalized medicine, but dynamic, adaptive, and precise human therapies” that adjust to the wound state moment by moment to provide greater resilience to wounded warfighters. “Wounds are living environments and the conditions change quickly as cells and tissues communicate and attempt to repair,” Sheehan said. “An ideal treatment would sense, process, and respond to these changes in the wound state and intervene to correct and speed recovery. For example, we anticipate interventions that modulate immune response, recruit necessary cell types to the wound, or direct how stem cells differentiate to expedite healing.”
“Wounds are living environments and the conditions change quickly as cells and tissues communicate and attempt to repair,” Sheehan said. “An ideal treatment would sense, process, and respond to these changes in the wound state and intervene to correct and speed recovery. For example, we anticipate interventions that modulate immune response, recruit necessary cell types to the wound, or direct how stem cells differentiate to expedite healing.”
DARPA anticipates that successful teams will include expertise in bioelectronics, artificial intelligence, biosensors, tissue engineering, and cellular regeneration. Further, DARPA encourages proposals that address healing following osseointegration surgery, which is often necessary to support the use of advanced prosthetics by wounded warfighters.